Coronavirus Vaccine - Personal Thoughts
In the last blog, I had analyzed the widely available data and accepted facts about Covid-19 disease and possible immunity against it in children and adults till 39 years of age.
Now there are two possibilities:
1. Either the coincidental vaccination for another disease has worked against the SARS-CoV-2 disease.
2. Or the kidneys and internal constitution against Covid-19 disease is so strong till 39 years that most infected patients get better with treatment. Since kidneys are stronger in young adults and work efficiently so the treatment works and fatality rates are lower.
But what if coincidental vaccination theory is logical and is assumed to be true? Then what is the next logical inference? It does explain the many asymptomatic individuals. In fact more than 50% infected individuals are silent carriers and get better without any drugs or treatment. So their body has antibodies to fight the SARS-CoV-2 virus. The virus does not affect the lungs and stays in upper respiratory area only.
So to understand vaccination for Covid-19 we have to understand the following:
1. How does vaccine normally work against a virus,
2. What is unique about the SARS-CoV-2 virus and
3. How are the experts world over creating the vaccine for Covid-19 disease?
If any similarities exist between this virus and other virus then it should be possible to have accidental immunization against the novel virus due to existing vaccine too.
The other radical thought is that despite dissimilarities in virus, if immune response from other vaccine can create antibodies which can fight off this novel virus antigens too. This is based on the memory created by a vaccine for creating antibodies against a given virus antigen.
Let us take a step back and see what SARS-CoV-2 virus is?


MA- Mandatory, NO - Neither mandatory nor recommended, RA - Recommended for All
So BCG vaccine is not being used everywhere. Although it holds interesting possibilities for boosting immunity against SARS-CoV-2 virus. Let us analyze each likely candidate highlighted above to see if there is a better alternative.
Pneumonia vaccine works against bacteria not virus.
DTP vaccine is against diphtheria bacteria, tetanus virus and Pertussis bacteria.
Tetanus virus shape is completely different from a corona virus. So it can be ruled out too.
Polio virus vaccine is likely candidate as the antibodies generated are present in respiratory tract too. So if they can protect against SARS-CoV-2 antigens too then yes children can be protected. But its effect lasts generally whole lifetime. You can check the link to below image from wiki also:

HIB vaccine is against bacteria infection. So we can remove this choice.
HPV is used for girls only and that too above 12 years of age. So this choice cannot be universally applied as of today.
MR vaccine holds interesting possibilities though. Measles causes an infection of the respiratory system and is caused by rubeola virus (measles virus). Measles virus is a negative sense single stranded virus with lipid envelope just like Corona virus. The antibodies to measles virus bind to the haemagluttinin protein. Please check this image of the spherical measles virus. It has striking resemblance to the SARS-CoV-2 corona virus.

This vaccine also protects against rubella virus (German measles). That virus also has top lipid layer called viral envelope. The core part is made up of protein and is also a positive-sense single stranded RNA virus similar to SARS-CoV-2 virus. Also its spherical viron has diameter of 50-70 nm which is strangely similar to the SARS-CoV-2 virus size. So MMR or its milder version MR vaccine can be tested as part of a small trial and then prescribed before Covid-19 vaccines are available in large numbers for the world population.
Tweet
1. Either the coincidental vaccination for another disease has worked against the SARS-CoV-2 disease.
2. Or the kidneys and internal constitution against Covid-19 disease is so strong till 39 years that most infected patients get better with treatment. Since kidneys are stronger in young adults and work efficiently so the treatment works and fatality rates are lower.
But what if coincidental vaccination theory is logical and is assumed to be true? Then what is the next logical inference? It does explain the many asymptomatic individuals. In fact more than 50% infected individuals are silent carriers and get better without any drugs or treatment. So their body has antibodies to fight the SARS-CoV-2 virus. The virus does not affect the lungs and stays in upper respiratory area only.
So to understand vaccination for Covid-19 we have to understand the following:
1. How does vaccine normally work against a virus,
2. What is unique about the SARS-CoV-2 virus and
3. How are the experts world over creating the vaccine for Covid-19 disease?
If any similarities exist between this virus and other virus then it should be possible to have accidental immunization against the novel virus due to existing vaccine too.
The other radical thought is that despite dissimilarities in virus, if immune response from other vaccine can create antibodies which can fight off this novel virus antigens too. This is based on the memory created by a vaccine for creating antibodies against a given virus antigen.
Let us take a step back and see what SARS-CoV-2 virus is?

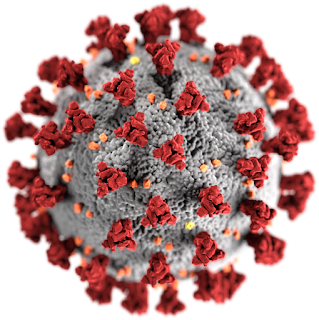
The virus has top lipid layer called viral envelope. The unique feature of this envelope are the spikes which give the name to this family of viruses called coronaviruses. The corona refers to this crown like appearance. The core part is made of protein and makes it a positive-sense single stranded RNA virus. The key part is its structure which can be seen in detail in this image. The spike glycoprotein S penetrates the human cell and paves way for infection. So this is important for understanding the attack of virus on human cells.
Now how is vaccination being invented for this virus? Are the scientists targeting the unique RNA code or its viral envelope? This question is very important as it holds the key to the body immune response (i.e. antibodies) and possible side effects of the vaccine.
The proteins in virus core part cannot be safely targeted by the artificial immunization easily or medicine treatment without killing human cells.
So the viral envelope is the key to generate body immune response through a vaccine.
The plant shaped spike protein, in the front, in the below image, is actually the experimental vaccine with inner core part of virus heavily deactivated or even absent in trials.

Why is that? Because the antibodies expected to be generated by the body will lock onto the spike protein of the actual virus. Then it will be impossible for the virus to latch onto human cells. And virus will be harmlessly discarded by the body.
In fact, the spike protein has a unique shape and is being used to make first vaccine mRNA-1273 and being tested at Seattle, USA. You can see the spike protein clearly here.
To summarize this virus is 50-200 nm in diameter with outer lipid layer forming an envelope using spike proteins. The vaccine is going to be made up of similar nano particles and envelope shapes. That way proper immune response can be triggered in body at the time of real infection with live virus and the body can fight it easily and recover.
Now coming to the original question, how come children and adults till 39 years are able to fight of viral infection of SARS-CoV-2 novel virus with no earlier immunization. But older adults and seniors are dying at higher rates? This is an anomaly and points to accidental immunity in children albeit with artificial means. Otherwise natural immunity would be greater in experienced adults who would have had already fought of many virus infections (flu etc), earlier.
In fact this thought has been captured not for the first time as a recent study by Indian Journal of Medical Sciences points to the lesser infections due to the BCG vaccine (used against Tuberculosis disease). Similar study by US scientists points to correlation of lower infection in India and Japan due to universal BCG vaccination policy.
But their conclusion is limited to lower number of people getting infected in India and the higher infections in Italy due to not having BCG vaccination there.
But there is one thing common between Japan, Italy, South Korea, China, Spain and India and that is very low fatality rates for children and young adults even after they get infected with virus. So Italy must have done something right in vaccination too. In fact this study, shows some interest in the BCG vaccine and curiosity about something else working right.
That other vaccine can instill proper antibody response if it is fighting a virus with similar mechanism if following holds true:
1. In particular the virus envelope should be similar to SARS-CoV-2 virus.
2. The vaccine for that should be used in Italy, Spain, Japan, India and South Korea on large scale.
We can look at the vaccination schedule in this link.
If we compare the vaccination program of various countries we have 7 vaccines being recommended for all children:

MA- Mandatory, NO - Neither mandatory nor recommended, RA - Recommended for All
So BCG vaccine is not being used everywhere. Although it holds interesting possibilities for boosting immunity against SARS-CoV-2 virus. Let us analyze each likely candidate highlighted above to see if there is a better alternative.
Pneumonia vaccine works against bacteria not virus.
DTP vaccine is against diphtheria bacteria, tetanus virus and Pertussis bacteria.
Tetanus virus shape is completely different from a corona virus. So it can be ruled out too.
Polio virus vaccine is likely candidate as the antibodies generated are present in respiratory tract too. So if they can protect against SARS-CoV-2 antigens too then yes children can be protected. But its effect lasts generally whole lifetime. You can check the link to below image from wiki also:
Hepatitis B vaccine is used in probably in all countries. But is it recommended for all (RA) or mandatory (M) or ordered by government act (A)?
Yes the picture is clearer on visiting this link. Hep-B vaccine is used in Japan, India, Spain, Italy and South Korea.This vaccine is used in UK and Australia too.
Also check the shape of Hepatitis B virus crown. Despite its different family and internal protein structure Hep-B spherical virus is very much similar to a coronavirus. Also Hep-B virus has top lipid layer and has spike proteins. Its diameter is 30-40 nm and its structure has been detailed here. This is similar to SARS-CoV-2 virus envelope.
Also Hep-B vaccine leads to generation of IgG antibodies by immune response. IgG is the main type of antibody found in blood and extracellular fluid, allowing it to control infection of body tissues by viruses. HIB vaccine is against bacteria infection. So we can remove this choice.
HPV is used for girls only and that too above 12 years of age. So this choice cannot be universally applied as of today.
MR vaccine holds interesting possibilities though. Measles causes an infection of the respiratory system and is caused by rubeola virus (measles virus). Measles virus is a negative sense single stranded virus with lipid envelope just like Corona virus. The antibodies to measles virus bind to the haemagluttinin protein. Please check this image of the spherical measles virus. It has striking resemblance to the SARS-CoV-2 corona virus.

This vaccine also protects against rubella virus (German measles). That virus also has top lipid layer called viral envelope. The core part is made up of protein and is also a positive-sense single stranded RNA virus similar to SARS-CoV-2 virus. Also its spherical viron has diameter of 50-70 nm which is strangely similar to the SARS-CoV-2 virus size. So MMR or its milder version MR vaccine can be tested as part of a small trial and then prescribed before Covid-19 vaccines are available in large numbers for the world population.
To summarize the two blogs:
1. There is definite evidence of artificial immunity (vaccine) working in children and young adults.
2. Based on difference in infection rate BCG vaccine is being researched further in Australia if it has contributed to low infection rate in Japan and India.
3. But the low death rates for children all across the world point to a vaccine which is already used in Italy, USA, UK and Australia too.
4. So we have 3 possible vaccine candidates for high immunity in children: Polio, MR and Hep-B. Now polio, measles and rubella point to disease of respiratory tract. So the two vaccines Polio and MR win over Hep-B vaccine. As Hep-B vaccine is for virus affecting liver so it looks doubtful. But the reduction in immunity with age happens in a more pronounced way for Hep-B vaccine. This fact matches with the data about age of coronavirus deaths.
This is a fairly small list and being existing approved vaccines they should be a ray of hope.
All this analysis is primarily based on Mathematics and little bit on Science. But a lot of this analysis is common sense which is guiding deeper look at lot of correlations in data.
The underlying motivations are:
1. Case fatality numbers vs age definitely tell a pattern of some successful vaccine working.
2. Taking the data from vaccination schedule and programs of various countries in the world point to 7 vaccines.
3. This list has been filtered based on similarities in structure of viruses further to 4 viruses and their vaccines only.
The basic question in your mind is how can another disease vaccine can work against a new disease? That is basically answered by looking at similarities in the virus. But the key is the immune response triggered by a vaccine. Are the antibodies generated versatile enough to work against two different viruses?
Other studies point to a fact about measles infection. It can reduce the range of antibodies even after recovery from measles infection. So MR vaccine booster shot can be a stronger candidate to prevent spread of coronavirus.
Hopefully it can help in further epidemiological research and analysis for a solution to this pandemic soon.
How? By first vaccinating the health workers who are in front line to defeat this pandemic. I mean they can be provided the booster shots from above discussed candidates after actual research by virologists.
Update 11 April 2020: There is an interesting update from CDC USA website.
Hospitalization rates increased with age, with a rate of 0.3 in persons aged 0–4 years, 0.1 in those aged 5–17 years, 2.5 in those aged 18–49 years, 7.4 in those aged 50–64 years, and 13.8 in those aged ≥ 65 years. Rates were highest among persons aged ≥ 65 years, ranging from 12.2 in those aged 65–74 years to 17.2 in those aged ≥ 85 years.
This again confirms some positive immunization in children aged 5 years or above till 49 years. Possibly suggesting an MR vaccine working. [It requires multiple doses and its last injection is given before 5 years.]
Update July 2020: MMR Vaccine Could Protect Against the Worst Symptoms of COVID-19


Comments
Post a Comment